With the second round of lymphatic filariasis Mass Drug Administration (MDA) campaign now underway, education remains key to getting patients to accept pills, says Dr Fabu Moses, the National Coordinator for the Elimination of Lymphatic Filariasis campaign.
Emphasis was placed on education, Moses told Stabroek News in an interview, after they realised many persons were not familiar with the pros and cons of consuming the pills that were being distributed in the MDA.
“The changes that we have done for this year’s campaign is that we have really tried to meet our audience better, engage our people and educate them well in advance before the MDA, so they get to internalise the information and understand what the MDA is all about,” she related.
According to Moses, while they were analysing the 2017 MDA campaign, they found many persons were not in tune with the objective of the campaign. In light of this, community health workers were given the task of educating persons.
Educational and interactive sessions were conducted in schools with parents and at local community health centres by community health workers.
“The workers from health centres went back into schools and met people on the road. They talked to the parents and teachers and answered questions and explained to them what it is,” Moses said. She added that many persons were confused by the term “dissent forms,” which has now changed to “refusal forms.”
“The dissent form—it was a bit difficult for them to really understand what was required of them. So we changed that and they are filling out a refusal form if they refuse,” Moses said. She pointed out that the form “gives all the information that we have out there. It tells them what MDA is about and what is targeted and the benefits and potential risk and how they occur.”
Overall success rate
This year’s MDA runs from October 1st to November 4th. Pill distributors have already started their work in Region Three, while Region Four is scheduled to start on Monday. Distribution in Regions Five and Ten is set to commence on October 15th and 22nd, respectively. During this period, persons can also visit their community health centres and request the pills. Mobile distribution tents are also expected to be erected across the targeted regions in high traffic area.
During the 2017 MDA, in Regions Three, Four, Five, and Ten, between one and eight percent of the population refused to accept the pills. Overall, 3 percent of the targeted population refused to take the pills.
In Region Three, which was the last region where the pill distribution was rolled out, Moses shared that many adults prevented their children between the ages of 2 to 5 years from consuming the pills. The refusal, she noted, resulted from the news of a child dying after consuming the pills.
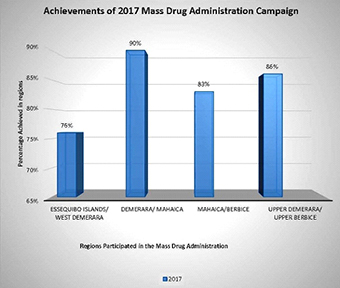
Last year’s campaign yielded an overall success rate of 86 percent, which Moses believes, resulted from the public awareness during the campaign period. In Region Four, 91 percent of the population consumed the pills, followed by Region Ten with 86 percent of the population taking the pills. In Region Five, the figure was at 81 percent while in Region Three, it was at 76 percent.
To achieve complete elimination of this neglected tropical disease, Dr Alexander Jean, a Malaria Control Specialist at the Pan American Health Organization (PAHO) said, every year at least 65 per cent of the population will have to receive the drug in order for complete elimination to be achieved. The 65 percent needs to be in the achieved in five consecutive years.

Lymphatic Filariasis, commonly known as elephantiasis and ‘big foot,’ occurs when filarial parasites are transmitted to humans through mosquitos’ bites. The World Health Organization (WHO) describes the sickness as a painful and profoundly disfiguring disease, which threatens persons of all ages in at-risk communities.
According to the WHO, “filarial infection can cause a variety of clinical manifestations, including lymphoedema of the limbs, genital disease (hydrocele, chylocele, and swelling of the scrotum and penis) and recurrent acute attacks, which are extremely painful and are accompanied by fever.”
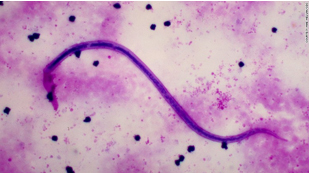
The thread-like nematode worms, known as filariae are transmitted through three types of worms – Wuchereria bancrofti, Brugia malayi and Brugia timori which are in turn, transmitted by the culex mosquito which is widespread across urban and semi-urban areas. The Anopheles, mainly found in rural areas, and Aedes, endemic in islands in the Pacific, are also two other types of mosquitoes that aids in the transmission of the disease.
The WHO’s website reported that 90 percent of cases resulted from infection by the Wuchereria bancrofti.
Moses explained that there is no way to detect the disease early as the symptoms only begin to show after years. At that time, it will be too late to reverse the illness and only treatment and care to deal with the enlarged tissues will be available.
“So it is important that all the at-risk persons in the regions take the pills that protect us. We can only have a success if at least 65% (of the population) take the pills. The more success we have is better because it means more protection for the people,” she emphasised. She indicated that prevention is the only cure.
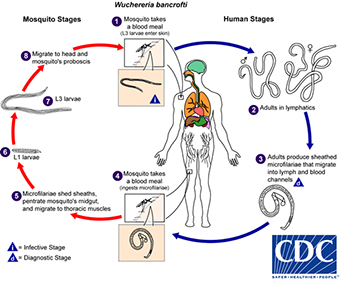
According to the WHO, the worms can live for approximately 6 to 8 years, and, during their lifetime, produce millions of microfilariae (immature larvae) that circulate in the blood.
The website explained that mosquitoes are infected with “microfilariae by ingesting blood when biting an infected host. Microfilariae mature into infective larvae within the mosquito.” It was further explained that when infected mosquitoes bite people, mature parasite larvae are deposited on the skin from where they can enter the body. The larvae then migrate to the lymphatic vessels where they develop into adult worms, thus continuing a cycle of transmission.
With Guyana signing on to efforts to eliminate neglected tropical diseases, it is racing to be filaria free by the year 2027.
The MDA is Guyana’s second approach to eliminating the neglected tropical disease through the distribution of filaria-eliminating drugs Albendazole and Diethylcarbamazine citrate (DEC) to citizens across the country. The drugs, according to the WHO, are deemed to be the safest and are the best approach to combating lymphatic filariasis.
Mapping
Meanwhile, to ensure that the MDA is effective across the country, a new mapping exercise is scheduled to begin next week in Regions One, Two, Six, Seven, Eight and Nine to assess if those regions are at risk.
Moses explained that the mapping exercise is necessary and “will be beneficial because it will help us to guide our intervention to those person who are particularly at risk.”
She explained that the updated mapping, which is being done in partnership with the Ministry of Public Health and the Pan-American Health Organisation, will determine the percentage of persons that are at risk and determine if it is endemic in the community.
During the mapping, blood samples will be taken and tested from persons between the ages of 6-14. This, Moses said, will show if communities are at risk. Focus, this time around will be placed on communities rather than regions as a whole. Moses noted that one at-risk community cannot determine the situation for the entire region.
“There was low percentage overall in those regions in 2001, but we never really check to see in clusters which particular one was at risk. Even though the percentage was low in the region, an area can be at risk. We are now looking to target at-risk clusters and focus on them. Once they are free, the region is free of filaria,” Moses underscored.
In Latin America, Dr William Adu-Krow, the director of PAHO, had said that Guyana is among four countries working to eliminate filariasis. It has been reported that apart from Guyana, lymphatic filariasis is still prevalent in Haiti, Dominican Republic and neighbouring Brazil.